Climber’s Elbow – aka the most frustrating injury
Just over 12 months ago I was doing a route toward the end of an endurance training session at the climbing wall when I popped out for a hold with my left hand. My forearms were already very fatigued and as I caught the hold and pulled through into a deep lock I felt a bursting strain at the elbow end of my forearm and in my wrist. This was toward the end of a period of training where I’d probably increased the volume and intensity both in parallel and too quickly. The following day I woke up and felt significant pain when straightening my arm. With that began probably my most frustrating year of rehabilitation from a climbing injury so far.
I rested for a week and then went back to the wall.
I’d stretched lots and the pain had generally subsided. Two routes into the warm up, it was clear that my body was telling me this was a bad idea and I told my belayer that was the end of my session. A further couple of weeks later, in Hamburg for New Year’s Eve, I went bouldering and despite my best intentions pushed it far too hard – the German bouldering team training problems were too well set to ignore. The result of this session was an inability to carry an empty shopping basket without pain.
Stupidity is doing the same thing over and over again and expecting a different result.
It was clearly time for a different approach. It’s taken twelve months of different opinions, methods and treatments, to get to the point where I can confidently say that recovery has been successful, and this blog is a summary of my learning through that journey, and of the reading I have done and the opinions I’ve heard. Don’t confuse it as professional medical advice, it’s not, but hopefully it will give you some hints and tips in getting over what is a really frustrating injury.
The first three bullets are the ones I felt are the most important, the further seven are secondary:
1. Diagnosis is important
 I had Medial Epicondylitis which is also known as Golfer’s elbow and Climber’s Elbow. This is not Tennis Elbow, which is on the other side of the elbow on the Lateral Epicondyle. If you have Tennis Elbow, then this blog is not going to help you!
I had Medial Epicondylitis which is also known as Golfer’s elbow and Climber’s Elbow. This is not Tennis Elbow, which is on the other side of the elbow on the Lateral Epicondyle. If you have Tennis Elbow, then this blog is not going to help you!
You can pinpoint the pain by placing your finger right on the insertion of the finger tendons into your elbow, essentially underneath the knobbly bit on the inside of your elbow, the Medial Epicondyle. There might also be secondary pain in your forearm.
If you have Golfer’s/Climber’s Elbow (Medial Epicondylitis) badly, it will hurt doing day to day tasks like washing your hair, carrying shopping and opening or closing doors.
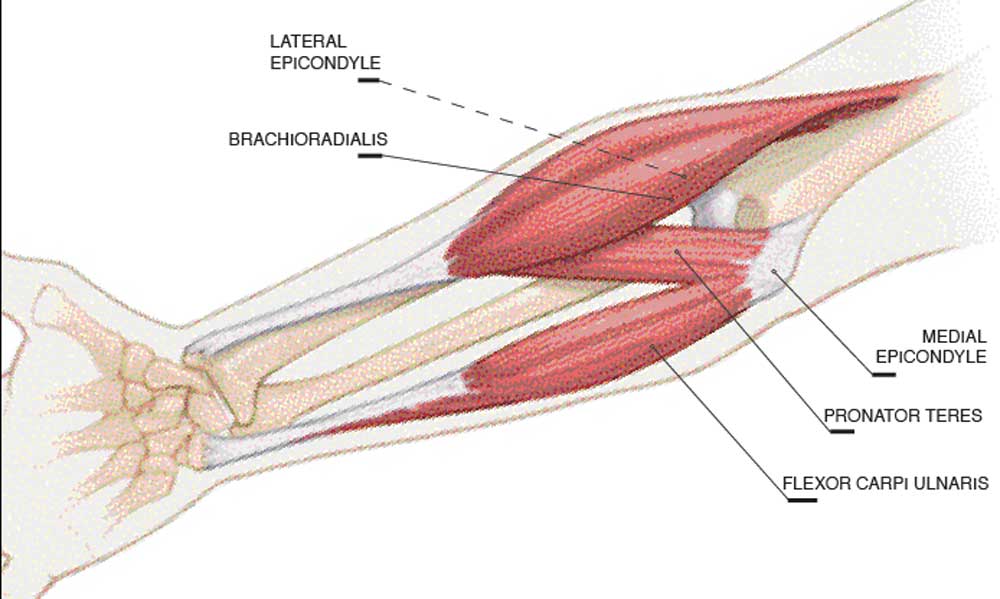
Beware, Pronator Teres and Medial Epicondylitis affect a very similar area of the elbow, as does Ulnar Nerve impingement. If you have any doubt about which injury you have then seek professional opinion. The eccentric exercises you will need to do are different and treating the wrong one can apparently make the other worse.
Tendonitis or Tendinosis
Tendonitis and tendinosis are different, both part of tendinopathy. Tendonitis is basically inflammation from overuse, tendinosis is more chronic pain/damage from poor healing and collagen damage.
You can generally get rid of tendonitis with a bit of rest, ice and stretching, over a couple of weeks, hence why many recommend rest initially. If rest doesn’t solve the issue, you may have tendinosis.
Climber’s Elbow is a form of tendinosis, which is crucially different from tendonitis. Unlike many injuries, Climber’s Elbow will not seemingly just go away with rest. Because it is caused by tendinosis, you need to break the poor cycle of healing and you need to be much more proactive with it than any other injury I’ve had. From reading a wide and varied number of articles, healing seems to take from 1 month to never depending on how severe it is, how chronic it is, but more importantly, how correct the treatment is. Crucially, healing tendonosis relies on your body creating enough collagen to repair the degenerated collagen in the tendon. According to studies this can take over 100 days.
2. You probably don’t need to stop climbing, but you might at first
Initially, my elbow was painful at rest. If that’s the case and it’s that severe, or you have pain that awakes you, as Dave Macleod recommends in Make or Break, it’s probably best to lay off all activity except for directly rehabilitative eccentric exercise (see below)
However, despite having had a whole year of this injury, I did manage to climb a fairly significant amount. But, I was careful.
I stopped climbing from January through to early May. Once I started climbing, I dropped my grade significantly and avoided certain styles of climbing. I completely laid off any chin ups and the campus board and have only recently very slowly reintroduced them.
I did not climb at the wall for 8 months. Instead I climbed, and seconded, lots of trad routes, which I knew I could physically climb quite comfortably, occasionally pushing the limit on things I knew were of a style that would not cause issues for my elbow.
Generally I avoided getting too pumped, over reaching, deep locks, deep undercuts, trad routes where you’d have to hang around for a long time on your arms to place gear, and very cruxy sport routes.
3. Do eccentric exercises, and do lots of them
These exercises are critical, and how you do them, how often you do them, and how you change them through recovery seems very important. My programme of eccentrics was a combination of Dr Julian Saunders blog advice, Dave Macleod’s method in his book Make or Break and nuggets of advice from Steve McClure and Rupert Davies. My methodology changed throughout the 6-7 months of doing eccentrics. Every time I reached a plateau I tweaked something to improve the healing.
The basic exercise
I took much of the information on this from here, but I have tweaked things as I got a feel for the injury as healing progressed.
You’re looking to lower a dumbbell weight in your hand slowly, resisting the fall of the weight as it eccentrically stretches your forearm under load. You can do this off the edge of a table, or as I tend to do, simply off the end of your knee, with the back of your forearm resting on your thigh.
Start with the weight resting on your leg with your knee at 90 degrees and your elbow at 90 degrees (the elbow angle can vary, but for an initial example use 90 degrees.)
 Your thumb should be below the dumbbell, not wrapped around, and you should tilt your hand slightly so your little finger is slightly higher than your thumb. This tilt seems to isolate the medial epicondylitis.
Your thumb should be below the dumbbell, not wrapped around, and you should tilt your hand slightly so your little finger is slightly higher than your thumb. This tilt seems to isolate the medial epicondylitis.

Over 4-5 seconds, gently and steadily lower the weight until you almost reach the limit of stretch. At that point take the force of the weight away with your other hand and lift back to the starting position.
Important: Lift the weight back up with your other hand. Do not do a wrist curl.
There’s many video examples of doing the exercise on youtube. Here’s one from John Ostrovoskis in Sheffield.
The elbow angle
The angle of your elbow whilst doing the exercise does make a difference on how much the injury is aggravated. In the early days of recovery my elbow would be aggravated at most angles. Most blogs suggest 90 – 120 degrees, but not beyond that. I started at 90 degrees, but as things improved the angles at which the elbow was aggravated slowly became more extreme. However the pain, when trying to climb or doing some daily tasks, had not gone away, so it was clear that more work and healing was required. If you’re not feeling discomfort, then tweak the angle. I did the exercises at the least extreme angle that aggravated the epicondyle. If the epicondyle is aggravated at both less than and greater than 90 degrees, then share the number repetitions equally between the acute (<90) and obtuse (>90) angles. Over time I felt the angles slowly move further apart until by the end of the recovery I was almost fully extended, and fully bent over.

Repetitions
I started doing 2 lots of 3 sets x 15 reps (90 total per day), one in the morning, one in the evening. I’d do this on both arms, alternating sets as you go so each arm. I did this initial repetition for about 6 weeks, but this soon didn’t seem to be enough. Rupert recommended doing 180 reps per day spread across 3 sets of 4 x 15 reps, breakfast, lunch and evening. Only after upping the repetitions to this level did I break through a plateau and suddenly accelerate progress.
I’d do this for 5 or 6 days out of 7 days, and would have a week off every 6 weeks.
Alongside increasing the weight, I would advise raising the reps slowly, don’t start with 180 reps, build up from 90 and learn how your injury feels as you go. Some mornings it feels ok, sometimes it feels really aggravated, just try and keep a track of what you did. Admittedly, sometimes I didn’t manage to do all the reps everyday for lots of reasons.
Weight
I started at 5kg as per many of the online and print guides. Whilst I could feel some aggravation in the elbow, it simply didn’t feel like enough weight to be having much effect.
After a couple of months, and feeling like I’d plateau’d, I spoke to Steve McClure and he simply recommended upping the weight “to whatever I could only just do 15 reps of.” A weight heavy enough so that after each group of sets you were close to failure (don’t drop the weight on your toe!), with only a marginal increase effort as you do more sets. The first set will obviously be easier than the last, so if you’re at 100% after the first set, the weight is too heavy. As a marker, I was at 85% at the end of the first set and 95-100% at the end of the last set. For me I got to 15kg in my last 6 weeks before the injury went away. Don’t forget, if you’re alternating sets on each arm, you’ll get about a minute rest between sets on each arm.
Summary
It seems counter intuitive, but for this to make progress, you have to aggravate the tendon and it will feel painful at times. Don’t overdo it, you’re not trying to win a prize for having a high pain threshold. The aggravation should be obvious, but manageable.
I didn’t record this exactly, but if you were to ask me what weight I used in each of the 6 week blocks, alongside the total number of reps per day, and the angle of the exercise, it will have looked something like this:
- 5kg – 90 reps at 90 degrees
- 6kg – 90 reps split between 100 and 70 degrees
- 8kg – 90 reps split between 120 and 50 degrees
- 12kg – 90 reps split between 150 and 45 degrees
- 14kg – 180 reps split between the extremes of extension/contraction (roughly 180 and 35)
- 15kg – 180 reps split between the extremes of extension/contraction (roughly 180 and 35)
Eccentric exercises are, in my opinion, the major driver of improvement, but you can certainly help accelerate their benefits with other things. Here are seven other things that either seemed to either promote the effect of the eccentric exercises, or prevented a plateau in improvement. None of these alone healed Climber’s Elbow, but all were useful in making sure rehabilitation was more effective.
4. Stretch after your eccentrics, and after climbing
2 simple stretches, 3 sets x 20 seconds of each after each dose of eccentrics
- Finger flexor stretch
- Finger extensor stretch
These stretches are well explained here: www.nicros.com/training/articles/essential-forearm-stretches/
Tom Randall suggested a type of yoga stretch on his blog. It didn’t rid me of the issue in 2 weeks(!), but it does seem to help ‘reset’ your elbow joint and get a deep stretch. Once I had started doing a programme of eccentrics that was working, and stretching using the regime above, this then didn’t seem to have the same ‘loosening off’ feeling as it did at first.
5. Ice after use
Whilst tendonosis is not technically due to inflammation, icing after the eccentric exercises (following stretching) and after climbing, or whenever there was a increase in discomfort seemed to have a positive effect compared to when I didn’t ice. Dr. Julian Saunders recommends heat, and no ice at all, but I did not try this. My personal view on icing is that with this injury we often have a tendency to do too much, and take a backward step in the process, and icing can limit any additional damage. If I were treating myself again, I would use a combination of ice and heat.
6. Sleeping position matters
Sleeping position does seem to affect the level of pain and aggravation in the injury. For me sleeping with a straightened arm meant waking up in pain, and taking a step backwards in healing.
At one point I tried using Kinesio tape. Whilst I don’t think it did anything for the injury itself, it did stop me sleeping with a straightened arm, and therefore allowed the healing to progress in an unexpected way.
7. Strengthen your core and shoulders
I aimed towards completing this, but don’t give yourself another injury!
8. Sort out your posture (i.e. step away from the desk)
Whilst it wasn’t the cause of the issue, computer work definitely aggravated the issue. Sitting at the computer all day is not good for you, full stop. For me, and for many, sometimes work demands that we have to spend hours at the desk.
Unfortunately climbers generally have terrible posture. When I focussed on good posture, sorted a good working position, and when possible, took a 5 min break every 25 minutes it was less aggravated by day to day work.
Whilst correcting posture alone will not solve Climber’s Elbow it did promote faster healing, and it’s certainly something that should help prevent future injury.
9. Massage
My usual course of action with a new minor sports injury is to go see Tim Budd. I also have an Armaid. It works, but it’s certainly not as effective as Tim, and I lacked the motivation and ability to use the Armaid the amount that I should have done. Massage definitely eased the pain in the elbow, and it sometimes seems like instant relief, but it was temporary relief on its own. Alongside a program of eccentrics I felt it broke the poor cycle of recovery and helped catalyse progress, but I didn’t think massage on its own will make it recover.
10. Warm up properly and don’t stop rehabilitation once you think it’s better
Warming up. Everyone throughout life tells you to warm up, from your primary school PE teacher to your Physiotherapist. One of the reasons you’re now probably at the Physiotherapist, paying to be treated, is because you ignored the advice of your primary school PE teacher. Warming up prevents injury, so do it.
- Raise the heart rate
- Increase mobility
- Start climbing and build up slowly
Secondly, don’t stop the rehabilitation just because it’s felt OK for a week. It takes about 100 days to produce new collagen, so reaching pain free status is just the start of recovery. If you just stop doing the eccentrics then Climber’s Elbow is probably going to creep back again pretty quickly.
A few other thoughts:
Just stay fit, do other things
Progress, as is often the case, seemed to accelerate when I was doing more exercise generally and cardio-work, unfortunately I also injured my ankle, so running had to stop for a while also. Swimming sometimes aggravated the elbow so take care with that.
Like all injuries, progress will not be linear
Progress can be slow, and especially so with an injury that takes so long to heal it can feel difficult to measure that progress. But one day you will go climbing and at the end of the day you’ll realise it hasn’t hurt. If you find it hard to mentally log progress, actually write down each day on a scale of 1 – 10 how painful it is and comment on the activity you have done.
Nutrition
Diet alone won’t cure you, but eating healthily will have an impact. I took fish oil, and many other have said the same, but I don’t think it’s a panacea! Cut back on the alcohol, if anything it affects your sleep and sleeping position.
Ibuprofen and Naproxen
It might take the pain away, but it won’t fix the problem, and like Dave Macleod says, it’ll probably tempt you to do more than you should. Do you really want to be taking NSAIDs for months at a time?
Professional Support
I’ve seen GPs, surgeons, physiotherapists, osteopaths and had an MRI.
After an MRI (which simply confirmed the issue and was probably unnecessary). The surgeon told me it would probably go away with rest and physiotherapy if I gave it a few more weeks. The GP prescribed Naproxen (an NSAID). Neither of which worked, nor did it go away in “a few more weeks.” Once I understood the injury the most effective support has been tiny nuggets of advice from climbers, mainly Steve McClure, Jordan Buys and Rupert Davies and I can’t thank them enough for what probably seemed like trivial bits of information at the time. And also from Tim Budd for deep muscle massage.
…and finally
One day you will wake up and your elbow won’t hurt. For me, it just disappeared one day, as quickly as it appeared. It’s a frustrating, niggly injury that never feels like it’s going to go away… and then it does. Good luck.
Other blogs etc
Here’s a list of further reading and resource that I have found helpful.
Dave Macleod: http://davemacleod.com/shop/makeorbreak.html
Tom Randall: https://tomrandallclimbing.wordpress.com/2012/11/23/golfers-elbow-a-possible-solution/
Dr Julian Saunders: http://drjuliansaunders.com/wp-content/uploads/2015/08/ri_dodgyelbow.pdf and http://www.rockandice.com/lates-news/rock-climbing-injury-dodgy-elbows-revisited
Nicros stretches: http://www.nicros.com/training/articles/essential-forearm-stretches/
Good summary of everything you’ve been doing John. Thoroughly agree that rest alone, and indeed massage on its own doesn’t get rid of this issue. There has been some good research on tendonopathies recently, and Professor Jill Cook is at the vanguard of it all. She has a couple of really accessible podcasts on the subject on the BJSM site.
Thanks Tim! It was a long road that one – thanks for you all your help and support with it.
I’ve had the same problem for the last 8 years and have managed it pretty well for the last 6 or so. I addition to your points I’d add another 3 that have been the most important for me for prevention/management. 1. Get good quality fish oil and eat it regularly. It has anti inflammatory properties and helped me to get rid of the pain within 2 weeks. 2. Electrical STEM massager. You can get one on ebay for $20. Don’t pay more for this, there are models that you can spend a few hundred on, but they don’t offer anything better. 3. Acupuncture. The doc I visited hooked me up to an electrical stimulator through the needles close to the medial epicondyle as well.
I wish you’d written this blog 2 years ago! I’ve been through the same process and this post has put in writing all my learnings, so thanks so much for taking the time to write it. I’m sure I’ll be using it again. In addition to your points, I agree with Vlad above, fish oil is very good specially to rebuild collagen. I’ve been told by a nutritionist that bone broth (if you can find it!) is very good for it too. Also, another natural helper is Alfafa powder, is loaded with minerals that are supposed to help with the rebuild process. I can’t tell for sure its effectiveness, but as soon as I started taking it I notice an immediate effect, but it could have been due to the exercises or a good timing in recovery. With the excentric exercises I did exactly the same one as you did, but added the flexbar too and a loads of thera band exercises to strengthen my shoulders, as my physio reckons my tendonisis keeps recurring because my shoulder is not stable enough. Anyways, I’m glad you are over the worse, time to crush!
Thanks Ramon. I actually took fish oil (and have now added a short bit into the blog – thanks for reminding me. I don[t think it’s a panacea, but with such a frustrating injury, every little helps. Along with a generally good diet. I found the flexbar more appropriate for pronator teres issues as it wasn’t as powerful as the out an out eccentrics. You’re absolutely right about shoulders, and also engaging your scapula better while climbing to get good “climbing posture”. Glad it’s recovered!
“Stupidity is doing the same thing again and again and expecting a different result” 🙂 possible typo there
Woops! Thanks for that! Fixed!
I suffered from this several times over the last 8+ years. I have tried all of your suggested remedies off and on for that time with some success, but nothing ever really lasting or consistent. I recently started lifting weights (for climbing) and am happy to report that ALL symptoms are completely gone. People are not joking when they say this (and other elbow issues) are due to muscular imbalances. Start lifting heavy weight and doing work on your triceps and biceps (shoulders will also help allot as well) and I assure you that you will be amazed at the result. Just remember – heavy weight and low reps with lots of rest between sets. I turned a years long struggle into a fix in less than four weeks of dedicated strengthening.
What exercises where you doing, specifically? Bench press (or dips?) can get shoulders and triceps. And then maybe some kind of open handed curl for biceps? I am wary of any kind of lat pull down as that’s replicating the exact motion of climbing that has gotten me in this trouble in the first place. Thanks for any suggestions!
It’s very interesting reading this, it’s almost a commentary on my last 10 months worth of elbow trouble. I did much the same and I was lucky to find out about eccentric exercises quite early from Dave’s book. I am now fixed, I hope.
Thanks, glad to hear the same worked for you.
Didn’t read all the comments so not sure if this was mentioned already but, try a workout tool called a Thera band flex bar. Do a workout called the reverse Tyler twist, has worked wonders for my golfers elbow.
Thanks, I didn’t find it strong enough to aggravate the issue. I do wonder also if it’s better suited to pronator teres issues, but not sure?
How did you manage your climbing load around all this tendon work? Im struggling with my second coming of the injury and sometimes the combination of climbing and eccentrics is just too much to handle. Should i just step away from the wall for a while and focus rehab?
I’m in a similar position after a lot of climbing over summer. It’s reared up a little bit, but keeping on top of it. If you’re in that situation it could be your climbing load is too high. I religiously do the eccentrics before and after the session, but tend to do lower volume sessions with a higher frequency (not always achievable if the wall isn’t close by or other commitments). Also very careful about the type of training when it’s flared. No campus, lower amount of finger boarding, and be careful on sessions like forced Boulder mileage where you’re getting powered down, pushing hard and technique can get sketchy toward the end of the set.
I have a weird(?) version of this tendonitis/tendonosis in that it doesn’t flare up until I stop climbing. I first noticed it after getting back into sets of pull-ups (used to do lots of them back in competitive swimming). I got pretty far along with my progress, then had to stop for a few weeks due to being out of town. Thus started my experiences with medial epicondylitis. It seems the only way for it to subside is to completely stop all climbing (and pull-up) activities. 6 months down the road, everything is healed, and I get going again with no problems for many months until something interrupts my schedule for a few weeks, and then, bam, the pain is back.
Of course the easy answer is to just never stop, but that isn’t always realistic.
Anyone else notice this kind of “rest” induced version of this nagging issue?
Thoughts or experiences?
Thanks!
P.s. – I have started doing the eccentric exercises mentioned above. I wouldn’t say the exercise aggravates it; just feels like a stretch. The next day, it does feel a little sore, however. Wonder if this is normal?
It is/was pretty normal for mine to flare up a bit with a change in climbing volume, so this doesn’t sound unreasonable. For me the longer term wins were from really spending training time focussing on posture and proper scapula engagement, and that transfers to really good pull up form.
The tendon feeling a little sore the morning after, is normal, definitely!
Understood. Likely your own flare ups with change in climbing volume were due to an increased workload, no? Funny that mine is always due to a sudden decrease in workload.
Ah well, I’ll stick with the eccentric stuff and hopefully it resolves. I feel that, like you, it may never be perfect again, just have to keep on top of it as it starts to get aggravated.
Thanks for creating this blog article and the info therein, much appreciated!
Oh that reminds me, speaking of muscular imbalances (was in someone else’s response post). Have you heard of or tried the simple resistance bands that wrap around all fingers and thumb at once? The exercise is to simply open the fingers and spread them out. This would be the opposing action to pinching/grasping that we perform in climbing and gripping. Activating and strengthening the lateral side of the elbow and forearm muscles to balance the medial ones, as it were. Wonder if these exercises will bear any fruit?
No any change in volume, up or down. Your muscles recover and strengthen when you rest (or reduce volume initially) and presumably then strain the tendon.
And yes, the resistance bands are great, use them most days, and as part of warm up. Lots of uses for them!